Conditions
ADHD

Treating Children With ADHD
In the past decade, prescriptions for Ritalin, a stimulant medication commonly used for attention deficit hyperactivity disorder (ADHD), increased five-fold, with 90 percent of all prescriptions worldwide consumed in the United States. As many parents grow leery of the traditional medical approach to ADHD, doctors of chiropractic are offering promising results with nondrug treatments that focus on postural muscles, nutrition and lifestyle changes that affect brain activity.
Some children may simply have difficulty learning certain subjects, but the current system—in a sense— prompts school officials to encourage their parents to have the children diagnosed with ADHD, says Dr. Scott Bautch, past president of the American Chiropractic Association (ACA) Council on Occupational Health. “The higher the number of disabled kids in the school, the more funding the school can apply for,” says Dr. Bautch.
Some teachers might also have difficulty with students who have a different style of learning, according to Dr. Bautch. If the child is a visual learner—and the teacher is not—perhaps the child is not being taught in a way he or she can learn. Before diagnosing the child with ADHD, Dr. Bautch recommends doctors talk to the child and the parents: “Is the child too active? Bored? Has dyslexia or a different learning pattern? It can be a behavior problem, problems at home, or frustrations with the teacher’s style,” explains Dr. Bautch. “If we went to a conference where the speakers taught in a way we can’t learn, we would be frustrated and would misbehave—we’d get up and leave or chat to the person sitting next to us.”
The traditional medical model, however, seems to follow the cookie-cutter principle. The diagnosis of ADHD is based on a questionnaire. But this is not enough, says Dr. Robert Melillo, a chiropractic neurologist. “True ADHD patients have other signs —tics, tremors, balance or postural problems, or unusual sensitivity to touch, movement, sights, or sounds.” Unfortunately, although medications can keep ADHD under control, they don’t cure it. Eighty percent of patients have ADHD features in adolescence, and up to 65 percent maintain them in adulthood.
Doctors of chiropractic and chiropractic neurologists offer a non-drug and non-invasive treatment alternative for ADHD patients that targets the underlying problems, not just symptoms. “Motor activity—especially development of the postural muscles—is the baseline function of brain activity. Anything affecting postural muscles will influence brain development. Musculoskeletal imbalance will create imbalance of brain activity, and one part of the brain will develop faster than the other, and that’s what’s happening in ADHD patients,” says Dr. Melillo.
Chiropractic neurologists are trained to identify the under functioning part of the brain and find treatments to correct the problem, to help that hemisphere grow. “On every patient, we perform a brain function exam,” says Dr. Frederick Carrick, president of the ACA Council on Neurology. “We test visual and auditory reflexes through, for example, flashing light in the eye, or asking patients to listen to music in one or the other ear.”
When the problem is identified, patients are placed on a treatment program—and most of the therapies can be done at home. “Patients are asked to smell certain things several times a day … or wear special glasses,” says Dr. Mark S. Smith, a chiropractic neurologist. “We also focus on their individual problems. Some children, for example, have difficulty with planning, organization, and coordination—so they benefit from timing therapies. They learn to clap or tap to the metronome, perform spinning and balancing exercises.”
Although currently no studies comparing chiropractic neurological and medical treatment for ADHD are available, chiropractic neurologists are compiling the data. “We test children before they start the treatment and then every three months,” says Dr. Melillo. “Within the first three months, the children get a two grade—level increase on average—which is pretty dramatic. With children on medications, the improvement in academic performance is short term and lasts only as long as they take the medication. Our programs change the brain function and the improvement doesn’t go away.”
If you or your loved one is diagnosed with ADHD or has the symptoms, ask your doctor of chiropractic if he or she has experience treating patients with the condition. Doctors of chiropractic are trained to identify neurological problems and find individual noninvasive treatment modalities. They can also assess your nutritional status and help you find the diet that will help you manage your condition.
Arthritis
Don’t Take Arthritis Lying Down
Years ago, doctors hardly ever told rheumatoid arthritis patients to “go take a hike” or “go for a swim.” Arthritis was considered an inherent part of the aging process and a signal to a patient that it’s time to slow down. However, recent research and clinical findings show that there is much more to life for arthritis patients than the traditional recommendation of bed rest and drug therapy.
What Is Rheumatoid Arthritis?
The word “arthritis” means “joint inflammation” and is often used in reference to rheumatic diseases. Rheumatic diseases include more than 100 conditions: gout, fibromyalgia, osteoarthritis, psoriatic arthritis, and many more. Rheumatic arthritis is also a rheumatic disease, affecting about 1 percent of the U.S. population (about 2.1 million people.) Although rheumatoid arthritis often begins in middle age and is more frequent in the older generation, young people and children can also suffer from it. Rheumatoid arthritis causes pain, swelling, stiffness, and loss of function in the joints.
Several features distinguish it from other kinds of arthritis:
- Tender, warm, and swollen joints.
- Fatigue, sometimes fever, and a general sense of not feeling well.
- Pain and stiffness that last for more than 30 minutes after a long rest.
- The wrist and finger joints closest to the hand are most frequently affected. Neck, shoulder, elbow, hip, knee, ankle, and feet joints can also be affected.
- The condition is symmetrical. If one hand is affected, the other one is, too.
- The disease can last for years and can affect other parts of the body, not only the joints.
Should Arthritis Patients Exercise?
Exercise is critical in successful arthritis management. It helps maintain healthy and strong muscles, joint mobility, flexibility, endurance, and helps control weight. Rest, on the other hand, helps to decrease active joint inflammation, pain, and fatigue. Arthritis patients need a good balance between the two: more rest during the active phase of arthritis, and more exercise during remission. During acute systematic flares or local joint flares, patients should put joints gently through their full range of motion once a day, with periods of rest. To see how much rest is best during flares, patients should talk to their health care providers. If patients experience unusual or persistent fatigue, increased weakness, a decrease in range of motion, an increase in joint swelling, or pain that lasts more than one hour after exercising, they need to talk to their health care providers.
Nutritional Recommendations
Nutrition may provide complementary support to arthritis medications. Some foods and nutritional supplements can be helpful in managing arthritis:
- Fatty-acid supplements like eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA), and gamma linolenic acid (GLA) Deep-sea fish, (salmon, tuna, herring, and halibut) are sources of EPA and DHA. Black currants and borage seed contain GLA.T
- Turmeric, ginger and nettle leaf extract
- A vegetarian or low-allergen diet
The benefits and risks of most of these agents are being researched. Before taking any dietary supplement, especially if you are using medication to control your condition, consult with your health care provider.
How Can Chiropractic Help?
If you suffer from rheumatoid arthritis, your doctor of chiropractic can help you plan an exercise program that will:
- Help you restore the lost range of motion to your joints.
- Improve your flexibility and endurance.
- Increase your muscle tone and strength.
Doctors of chiropractic can also give you nutrition and supplementation advice that can be helpful in controlling and reducing joint inflammation.
Asthma
 What is Causing the Asthma Epidemic?
What is Causing the Asthma Epidemic?
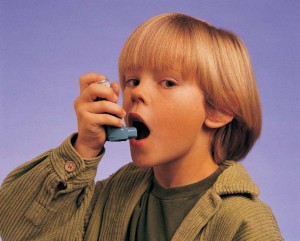
In the United States, asthma cases have increased by more than 60 percent since the early 1980s, and asthma-related deaths have doubled to 5,000 a year. What is causing the asthma epidemic and what can we do to stem the tide?
People in their 30s and older can remember that when they were young, it was very unusual for even one child in school to have asthma. Schoolchildren now often know several kids with asthma in a single class. The rapid increase in the number of young people with asthma was brought home to Dr. Scott Bautch, member of the American Chiropractic Association’s (ACA) Council on Occupational Health, when he went to a football game with his 13-year-old son: “Someone on the field had a breathing problem. It was hard to see whose son it was, and 15 parents ran to the field with inhalers.”
What Causes Asthma?
So far, researchers don’t know why cases of asthma are increasing at such an alarming rate. They hypothesize that a combination of genetics and some nonhereditary factors— such as increased environmental exposure to potential allergens — plays a role. “Thirty years ago, Windex was the only cleaning solvent used by a few people. Now, we have a special cleaning solvent for every object,” says Dr. Bautch. “In addition, furniture and carpets are produced with formaldehyde as a preservative, and people breathe it,” he says.
Decreased air quality is coupled with the allergy-friendly modern house design, says Dr. William E. Walsh, MD, FACC, an allergist practicing in Minnesota: “Fifty years ago we lived in old, drafty houses, and the breeze dried and freshened the air, and cleared out mold and other allergens. Nowadays, our super-insulated houses don’t breathe adequately. Making basements into a living space increases mold exposure because mold grows in any basement.”
Food has become another source of exposure to allergens. “Food manufacturers put more preservatives in foods now to store them longer,” says Dr. Bautch. Researchers hypothesize that an increase in vaccinations, cesarean births, and antibiotic intake may be playing a role, too.
How Can Asthma Be Treated?
Asthma is a chronic disease; it can’t be cured —only controlled. For best treatment results, both the primary care physician and an asthma specialist, such as an allergist or pulmonologist, should be involved. According to experts interviewed for the article, the treatment program, in addition to medication intake, should include reducing exposure to the substances that induce acute episodes and identifying specific allergens that affect the patient.
Non-Allergen Causes of Asthma
Allergens aren’t the only culprit of asthma attacks. Stress factors — such as moving to a new home, or changing jobs — may induce or aggravate asthma attacks. Even emotional expressions such as fear, anger, frustration, hard crying, or laughing can cause an attack as well. To reduce the patient’s stress level and improve the patient’s quality of life, alternative treatments should be incorporated into the treatment program. Various relaxation techniques, such as biofeedback, meditation, yoga, and stress management, as well as massage, chiropractic manipulation, breathing exercises, and acupuncture can be helpful.
Chiropractic Care Can Help
“Doctors of chiropractic can give a full-scale evaluation to asthma patients; assess their physical and neurological status, their lifestyle, diet, and stressors; and help the patients increase motor coordination, and improve the work of respiratory and gut muscles to increase the quality of life,” says Dr. Gail Henry, a chiropractic neurologist, who practices in Houston, Texas. “Doctors of chiropractic can be a great addition to the healthcare team treating the asthma patient.”
Talk to your doctor of chiropractic about other ways to improve your quality of life. Doctors of chiropractic are trained and licensed to examine and treat the entire body with emphasis on the nervous and musculoskeletal systems. They also help people lead healthier lives by focusing on wellness and prevention.
Back Pain
 Does Back Pain Go Away on Its Own?
Does Back Pain Go Away on Its Own?
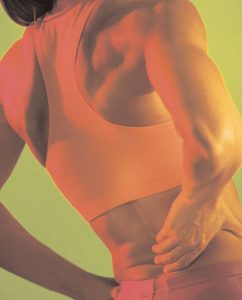
Eighty percent of people suffer from back pain at some point in their lives. Back pain is the second most common reason for visits to the doctor’s office, outnumbered only by upper-respiratory infections. Most cases of back pain are mechanical or non-organic—not caused by serious conditions, such as inflammatory arthritis, infection, fracture, or cancer.
What Causes Back Pain?
The back is a complicated structure of bones, joints, ligaments, and muscles. You can sprain ligaments, strain muscles, rupture disks, and irritate joints, all of which can lead to back pain. While sports injuries or accidents can cause back pain, sometimes the simplest of movements—for example, picking up a pencil from the floor— can have painful results. In addition, arthritis, poor posture, obesity, and psychological stress can cause or complicate back pain. Back pain can also directly result from disease of the internal organs, such as kidney stones, kidney infections, blood clots, or bone loss.
Back injuries are a part of everyday life, and the spine is quite good at dealing with these often “pulled” muscles. These very minor injuries usually heal within 1 or 2 days. Some pain, however, continues. What makes it last longer is not entirely understood, but researchers suspect that the reasons may include stress, mood changes, and the fear of further injury that may prevent patients from being active. In addition, sometimes a painful injury or disease changes the way the pain signals are sent through the body, and, even after the problem has gone away or is inactive, the pain signals still reach the brain. It is as if the pain develops a memory that keeps being replayed.
Will Back Pain Go Away on Its Own?
Until recently, researchers believed that back pain would heal on its own. We have learned, however, that this is not true. A recent study showed that when back pain is not treated, it may go away temporarily, but will most likely return. The study demonstrated that in more than 33% of the people who experience lowback pain, the pain lasts for more than 30 days. Only 9% of the people who had low-back pain for more than 30 days were pain free 5 years later.
Another study looked at all of the available research on the natural history of low-back pain. The results showed that when it is ignored, back pain does not go away on its own, but continues to affect people for long periods after it first begins.
What Can I Do to Prevent Long-Term Back Pain?
If your back pain is not resolving quickly, visit your doctor of chiropractic. Your pain will often result from mechanical problems that your doctor of chiropractic can address. Many chiropractic patients with relatively long-lasting or recurring back pain feel improvement shortly after starting chiropractic treatment. The relief is often greater after a month of chiropractic treatment than after seeing a family physician. Chiropractic spinal manipulation is a safe and effective spine pain treatment. It reduces pain, decreases medication, rapidly advances physical therapy, and requires very few passive forms of treatment, such as bed rest.
How Can I Prevent Back Pain?
- Don’t lift by bending over. Instead, bend your hips and knees and then squat to pick up the object. Keep your back straight, and hold the object close to your body.
- Don’t twist your body while lifting.
- Push, rather than pull, when you must move heavy objects.
- If you must sit for long periods, take frequent breaks and stretch.
- Wear flat shoes or shoes with low heels.
- Exercise regularly. An inactive lifestyle contributes to lower-back pain.
Carpal Tunnel Syndrome
Carpal tunnel syndrome (CTS) is the most expensive of all work-related injuries. Over his or her lifetime, a carpal tunnel patient loses about $30,000 in medical bills and time absent from work.
CTS typically occurs in adults, with women 3 times more likely to develop it than men. The dominant hand is usually affected first, and the pain is typically severe. CTS is especially common in assembly-line workers in manufacturing, sewing, finishing, cleaning, meatpacking, and similar industries. Contrary to the conventional wisdom, according to recent research, people who perform data entry at a computer (up to 7 hours a day) are not at increased risk of developing CTS.
What Is CTS?
CTS is a problem of the median nerve, which runs from the forearm into the hand. CTS occurs when the median nerve gets compressed in the carpal tunnel—a narrow tunnel at the wrist—made up of bones and soft tissues, such as nerves, tendons, ligaments, and blood vessels. The compression may result in pain, weakness, and/or numbness in the hand and wrist, which radiates up into the forearm. CTS is the most common of the “entrapment neuropathies”—compression or trauma of the body’s nerves in the hands or feet.
What Are the Symptoms?
Burning, tingling, itching, and/or numbness in the palm of the hand and thumb, index, and middle fingers are most common. Some people with CTS say that their fingers feel useless and swollen, even though little or no swelling is apparent. Since many people sleep with flexed wrists, the symptoms often first appear while sleeping. As symptoms worsen, they may feel tingling during the day. In addition, weakened grip strength may make it difficult to form a fist or grasp small objects. Some people develop wasting of the muscles at the base of the thumb. Some are unable to distinguish hot from cold by touch.
Why Does CTS Develop?
Some people have smaller carpal tunnels than others, which makes the median nerve compression more likely. In others, CTS can develop because of an injury to the wrist that causes swelling, over-activity of the pituitary gland, hypothyroidism, diabetes, inflammatory arthritis, mechanical problems in the wrist joint, poor work ergonomics, repeated use of vibrating hand tools, and fluid retention during pregnancy or menopause.
How Is It Diagnosed?
CTS should be diagnosed and treated early. A standard physical examination of the hands, arms, shoulders, and neck can help determine if your symptoms are related to daily activities or to an underlying disorder. Your doctor of chiropractic can use other specific tests to try to produce the symptoms of carpal tunnel syndrome.
The most common are:
- Pressure-provocative test. A cuff placed at the front of the carpal tunnel is inflated, followed by direct pressure on the median nerve.
- Carpal compression test. Moderate pressure is applied with both thumbs directly on the carpal tunnel and underlying median nerve at the transverse carpal ligament. The test is relatively new.
Laboratory tests and x-rays can reveal diabetes, arthritis, fractures, and other common causes of wrist and hand pain. Sometimes lectrodiagnostic tests, such as nerveconduction velocity testing, are used to help confirm the diagnosis. With these tests, small electrodes, placed on your skin, measure the speed at which electrical impulses travel across your wrist. CTS will slow the speed of the impulses and will point your doctor of chiropractic to this diagnosis.
What Is the CTS Treatment?
Initial therapy includes:
- Resting the affected hand and wrist
- Avoiding activities that may worsen symptoms
- Immobilizing the wrist in a splint to avoid further damage from twisting or bending
- Applying cool packs to help reduce swelling from inflammations
Some medications can help with pain control and inflammation. Studies have shown that vitamin B6 supplements may relieve CTS symptoms. Chiropractic joint manipulation and mobilization of the wrist and hand, stretching and strengthening exercises, soft-tissue mobilization techniques, and even yoga can be helpful. Scientists are also investigating other therapies, such as acupuncture, that may help prevent and treat this disorder.
Occasionally, patients whose symptoms fail to respond to conservative care may require surgery. The surgeon releases the ligament covering the carpal tunnel. The majority of patients recover completely after treatment, and the recurrence rate is low. Proper posture and movement as instructed by your doctor of chiropractic can help prevent CTS recurrences.
Chronic Pain & Depression
 Pain serves an important function in our lives. When you suffer an acute injury, pain warns you to stop the activity that is causing the injury and tells you to take care of the affected body part.
Pain serves an important function in our lives. When you suffer an acute injury, pain warns you to stop the activity that is causing the injury and tells you to take care of the affected body part.
Chronic pain, on the other hand, persists for weeks, months, or even years. Some people, often older adults, suffer from chronic pain without any definable past injury or signs of body damage. Common chronic pain can be caused by headaches, the low back, and arthritis. Unfortunately, there is scant objective evidence or physical findings to explain such pain.
Until recently, some doctors who could not find a physical cause for a person’s pain simply suggested that it was imaginary—“all in your head.” This is unfortunate because we know that all pain is real and not imagined, except in the most extreme cases of psychosis. Emerging scientific evidence is demonstrating that the nerves in the spinal cord of patients with chronic pain undergo structural changes.
Psychological and social issues often amplify the effects of chronic pain. For example, people with chronic pain frequently report a wide range of limitations in family and social roles, such as the inability to perform household or workplace chores, take care of children, or engage in leisure activities. In turn, spouses, children, and co-workers often have to take over these responsibilities. Such changes often lead to depression, agitation, resentment, and anger for the pain patient and to stress and strain in family and other social relationships.
How is depression involved with chronic pain?
Depression is the most common emotion associated with chronic pain. It is thought to be 3 to 4 times more common in people with chronic pain than in the general population. In addition, 30 to 80% of people with chronic pain will have some type of depression. The combination of chronic pain and depression is often associated with greater disability than either depression or chronic pain alone.
People with chronic pain and depression suffer dramatic changes in their physical, mental, and social well-being—and in their quality of life. Such people often find it difficult to sleep, are easily agitated, cannot perform their normal activities of daily living, cannot concentrate, and are often unable to perform their duties at work. This constellation of disabilities starts a vicious cycle—pain leads to more depression, which leads to more chronic pain. In some cases, the depression occurs before the pain.
Until recently, we believed that bed rest after an injury was important for recovery. This has likely resulted in many chronic pain syndromes. Avoiding performing activities that a person believes will cause pain only makes his or her condition worse in many cases.
Depression associated with pain is powerful enough to have a substantial negative impact on the outcome of treatment, including surgery. It is important for your doctor to take into consideration not only biological, but also psychological and social issues that pain brings.
What is the treatment for chronic pain and depression?
The first step in coping with chronic pain is to determine its cause, if possible. Addressing the problem will help the pain subside. In other cases, especially when the pain is chronic, you should try to keep the chronic pain from being the entire focus of your life.
- Stay active and do not avoid activities that cause pain simply because they cause pain. The amount and type of activity should be directed by your doctor, so that activities that might actually cause more harm are avoided.
- Relaxation training, hypnosis, biofeedback, and guided imagery, can help you cope with chronic pain. Cognitive therapy can also help patients recognize destructive patterns of emotion and behavior and help them modify or replace such behaviors and thoughts with more reasonable or supportive ones.
- Distraction (redirecting your attention away from chronic pain), imagery (going to your “happy place”), and dissociation (detaching yourself from the chronic pain) can be useful.
- Involving your family with your recovery may be quite helpful, according to recent scientific evidence.
Feel free to discuss these or other techniques with your doctor of chiropractic. He or she may suggest some simple techniques that may work for you or may refer you to another health care provider for more indepth training in these techniques.
Cold and Flu
 With cold weather knocking on the door, many are concerned about falling victim to colds and flu. Flu vaccine—the most effective way to prevent the flu, according to the Centers for Disease Control and Prevention—remains a controversial subject. First, most flu vaccines still contain thimerosal, a mercury based preservative. Second, because of the unpredictability of flu strains, the available vaccine often doesn’t match the strain of flu that hits the population.
With cold weather knocking on the door, many are concerned about falling victim to colds and flu. Flu vaccine—the most effective way to prevent the flu, according to the Centers for Disease Control and Prevention—remains a controversial subject. First, most flu vaccines still contain thimerosal, a mercury based preservative. Second, because of the unpredictability of flu strains, the available vaccine often doesn’t match the strain of flu that hits the population.
But even if the vaccine corresponds with the circulating flu strain, it is not that effective. A recent study found that the overall effectiveness of vaccines against flu-like illness in the elderly was 23 percent when vaccine matching was good, and “not significantly different from no vaccination when matching was poor or unknown.” Well-matched vaccine, however, may effectively prevent pneumonia and decrease hospitalization rates due to pneumonia or flu.
Recent research shows that the best protection from flu may be flu itself. In the past 20 years, deaths from flu in the elderly have decreased. At the same time, flu vaccination has increased by 45 to 50%. Researchers concluded, that flu vaccine didn’t help decrease deaths from flu—people simply acquired natural immunity to the emerging strain of flu. Because of this, many are looking into natural ways to prevent viruses.
Garlic
Garlic has been used as a health food for more than5,000 years and is touted for its antibiotic properties and effect on general immunity.
A recent study found that a group of people treated with an allicin-containing garlic supplement for a period of 12 weeks between November and February had In the group treated with the garlic supplement, 24 people came down with the common cold, which lasted for 1.52 days, compared with 65 people in the no treatment group who had colds that lasted 5 days on average.
Garlic therapy should be discontinued at least two weeks prior to surgery to prevent excessive bleeding. People on anticoagulants should consult their physicians.
Tea
Green and black teas have been studied for their effects on the cardiovascular system and cancer. A recent Harvard study looked at tea’s role in boosting the immunity system. Participants who drank five cups of black tea a day for 2 to 4 weeks increased their levels of interferon, an important immune defense hormone—up to 4 times normal levels. Drinking the same amount of coffee for 12 weeks produced no such effects. The researchers suggest that the key was in Ltheanine, a substance in tea that increases immune response in fighting bacteria, infection, viruses and fungi. Excessive doses may cause insomnia, headache, dizziness, and diarrhea.
Vitamin C
The role of vitamin C in the prevention and treatment of respiratory infections has been widely researched. Some studies suggest that vitamin C can affect the duration or severity of symptoms. Others have shown no effect on the symptoms, but suggested that vitamin C can reduce susceptibility to colds.
A recent study compared 29 clinical trials in which participants received 200 mg or more of vitamin C daily. The researchers found that vitamin C prevented flu or colds in people who were exposed to “brief periods of severe physical exercise and/or cold environments.” In those who regularly take vitamin C, they concluded that vitamin C plays some role in their defense mechanisms, helping them to recover from their colds faster and reducing the severity of symptoms. People with kidney disease should not use vitamin C.
Echinacea
Echinacea has been widely used to prevent and treat colds. Research on the plant, however, has produced conflicting results. A recent study that focused on 3 preparations from echinacea root found no clinically significant effects on the common cold. The critics of the study believe, however, that the dose of 900 mg per day was too low. Echinacea treatment may lead to minor and uncommon abdominal upset, nausea and dizziness. It may be contraindicated in people with autoimmune conditions or HIV.
Zinc Lozenges
Zinc lozenges are another home remedy for fighting winter viruses. Although research on this remedy is conflicting, a recent study on zinc gluconate glycine lozenges in school-aged children showed shorter cold duration and fewer colds with the therapy. Zinc lozenges, however, come in different formulations, and more research is needed to assess their effectiveness. In addition, long-term use of zinc lozenges may lead to problems, including impairing the body’s immune responses. Excessive zinc in the diet can lead to copper deficiency and may also decrease the levels of HDL (“good”) cholesterol in the blood.
Additional Remedies
Research indicates that chronic stress may substantially increase the risk of catching cold and stress management reduces the duration of flu and colds.
Acupuncture may be effective against preventing and curing the common cold, as well. Many chiropractors have also noticed that chiropractic adjustments have helped prevent or reduce the duration of their patients’ colds. Preliminary results of an ongoing chiropractic study show that chiropractic may increase immunoglobulin A levels and that it decreases the levels of glucocorticoid cortisol, a major component of stress.
Diabetes
 Diabetes is a severe health condition that can cause life-altering and even life-threatening problems, such as slow wound healing and nerve disorders. It can also complicate problems in muscles, bones, and joints. Diabetes results from an excessive buildup of glucose in your bloodstream. Glucose, or blood sugar, which the body gets from food and also manufactures in the liver and muscles, is a substance the body uses for energy and nutrition. To control glucose levels in your blood, the body uses insulin, a substance produced by the pancreas. An imbalance in this system can cause pre-diabetes or diabetes.
Diabetes is a severe health condition that can cause life-altering and even life-threatening problems, such as slow wound healing and nerve disorders. It can also complicate problems in muscles, bones, and joints. Diabetes results from an excessive buildup of glucose in your bloodstream. Glucose, or blood sugar, which the body gets from food and also manufactures in the liver and muscles, is a substance the body uses for energy and nutrition. To control glucose levels in your blood, the body uses insulin, a substance produced by the pancreas. An imbalance in this system can cause pre-diabetes or diabetes.
In most people, normal blood glucose levels range from 80 to 120. The levels vary depending on the time of day and how long it has been since you’ve eaten. Levels can go as high as 180 within 2 hours after a meal. Pre-diabetes is excess blood glucose that is not severe enough to be called diabetes. The mild-to-moderate abnormal blood glucose levels of pre-diabetes can make you more likely to develop type 2 diabetes, stroke, and heart disease.
Types of Diabetes
There are two main types of the disease. Type 1 diabetes, formerly called juvenile or insulin-dependent diabetes, usually begins in childhood to early adulthood. It results from destruction of insulin-producing cells in the pancreas. When the body destroys these cells, insulin levels in the blood become too low to properly manage blood sugar.
Type 2 diabetes is also called adult-onset diabetes or non-insulin-dependent diabetes. This condition results from insulin resistance—the inability of body tissues to properly utilize insulin produced by the pancreas. The pancreas compensates by producing more insulin, but eventually it cannot keep up with the demand, especially after meals. Obesity, poor diet, and lack of exercise predispose you to developing type 2 diabetes.
A less common form of the disease is called gestational diabetes. It occurs, secondary to hormonal changes, in pregnant women during the late stages of pregnancy and usually resolves after the birth of the baby. It is important to remember, however, that gestational diabetes makes a woman more likely to develop type 2 diabetes later in life.
Managing Glucose Levels
With diabetes, uncontrolled glucose levels can lead to serious problems with vision, kidney function, nerve dysfunction, and blood vessels, including heart attack and stroke. In fact, people with diabetes have approximately twice the risk of stroke and heart attack faced by the general public.
In a nutshell, to manage glucose levels, you should exercise regularly, eat a healthful balanced diet, and maintain a healthy body weight.
Physical activity helps control blood glucose levels in both healthy adults and in diabetics. Aerobic exercise, such as walking, swimming, dancing, and riding a bicycle, appears to be most beneficial. What that does is raise your heart rate, helping to not only control blood glucose but also prevent heart attack and stroke. You can get some exercise by house cleaning or doing yard work, such as gardening. Physical activity helps diabetic patients maintain a healthy body weight, helps insulin lower the blood glucose levels, and gives patients more energy. Before you start an exercise program, consult with your doctor to make sure that the exercise program is tailored to fit your specific needs.
It’s also important to eat foods that are generally low in fat—and when fats are eaten, aim for “good” ones, such as those found in olive oil, fish, and other products. People with diabetes don’t need to eat special foods but should avoid foods that contain large amounts of saturated and/or trans fats. They should also avoid eating too many processed sugars, but instead choose complex carbohydrates such as those found in fruits and vegetables. The benefits of this type of healthy diet can extend beyond blood sugar control and diabetes prevention to help prevent heart attack and stroke.
Maintaining a healthy body weight usually comes naturally from good eating habits and regular exercise. Some even suggest that these two steps alone influence the prevalence of diabetes and the maintenance of healthy blood sugar levels.
Ear Infections
 Ear problems can be excruciatingly painful, especially in children. With 10 million new cases every year, ear infections (otitis media) are the most common illness affecting babies and young children and the number one reason for visits to the pediatrician—accounting for more than 35 percent of all pediatric visits.
Ear problems can be excruciatingly painful, especially in children. With 10 million new cases every year, ear infections (otitis media) are the most common illness affecting babies and young children and the number one reason for visits to the pediatrician—accounting for more than 35 percent of all pediatric visits.
Almost half of all children will have at least one middle ear infection before they’re a year old, and two-thirds of them will have had at least one such infection by age 3. The symptoms can include ear pain, fever, and irritability. Otitis media can be either bacterial or viral in origin, and frequently results from another illness such as a cold. For many children, it can become a chronic problem, requiring treatment year after year, and putting the child at risk of permanent hearing damage and associated speech and developmental problems.
Standard treatment for most cases of otitis media is with antibiotics, which can be effective if the culprit is bacterial (antibiotics, of course, do nothing to fight off viruses). But, according to many research studies, antibiotics are often not much more effective than the body’s own immune system. And repeated doses of antibiotics can lead to drug-resistant bacteria that scoff at the drugs, while leaving the child screaming in pain.
Frequent ear infections are also the second most common reason for surgery in children under 2 (with circumcision being the first). In severe cases—for example, when fluids from an ear infection haven’t cleared from the ear after several months, and hearing is affected—specialists sometimes prescribe myringotomy and tympanostomy, more commonly known as “ear tubes.” During the surgical procedure, a small opening is made in the eardrum to place a tube inside. The tube relieves pressure in the ear and prevents repeated fluid buildup with the continuous venting of fresh air. In most cases, the membrane pushes the tube out after a couple of months and the hole in the eardrum closes. Although the treatment is effective, it has to be repeated in some 20 to 30 percent of cases. And this kind of surgery requires general anesthesia, never a minor thing in a small child. If the infection persists even after tube placement and removal, children sometimes undergo adenoidectomy (surgical removal of the adenoids)—an option that is effective mostly through the first year after surgery.
Before yet another round of “maybe-they’ll-work-andmaybe- they-won’t” antibiotics or the drastic step of surgery, more parents are considering chiropractic to help children with chronic ear infections. Dr. Joan Fallon, a chiropractor who practices in Yonkers, New York, has published research showing that, after receiving a series of chiropractic adjustments, nearly 80 percent of the children treated were free of ear infections for at least the six-month period following their initial visits (a period that also included maintenance treatments every four to six weeks). “Chiropractic mobilizes drainage of the ear in children, and if they can continue to drain without a buildup of fluid and subsequent infection, they build up their own antibodies and recover more quickly,” explains Dr. Fallon. She’d like to see her pilot study used as a basis for larger-scale trials of chiropractic as a therapeutic modality for otitis media.
Dr. Fallon uses primarily upper-cervical manipulation on children with otitis media, focusing particularly on the occiput, or back of the skull, and atlas, or the first vertebra in the neck. “Adjusting the occiput, in particular, will get the middle ear to drain. Depending on how chronic it’s been and on where they are in their cycle of antibiotics, children generally need to get through one bout of fluid and fight it off themselves.” That means, for the average child, between six and eight treatments.
If a child’s case is acute, Dr. Fallon will check the ear every day, using a tympanogram to measure the ear and track the movement of the eardrum to make sure that it’s draining. “I’ll do adjustments every day or every other day for a couple of days if they’re acute, and then decrease frequency over time.”
Dr. Fallon, whose research garnered her the acclaim of childrearing magazines like Parenting and Baby Talk, often sees great success when she treats a child for otitis media. “Once they fight it themselves, my kids tend to do very well and stay away from ear infections completely. Unless there are environmental factors like smoking in the house, an abnormally shaped Eustachian tube, or something like that, they do very well,” she says.
“I have two large pediatric groups that refer to me on a regular basis. In the winter, when otitis is most prevalent, I see five or six new children each week from each group,” says Dr. Fallon. “It’s safe and effective and something that parents should try, certainly before inserting tubes in their children’s ears.”
Chiropractic Care Can Help
Talk to your doctor of chiropractic about your child’s ear infections. Doctors of chiropractic are licensed and trained to diagnose and treat patients of all ages and will use a gentler type of treatment for children. In addition, doctors of chiropractic can also prescribe exercises designed to help children develop strong muscles, along with instruction in good nutrition, posture and sleeping habits.
Fibromyalgia
 If you or your loved ones have been diagnosed with fibromyalgia, you may be wondering what the disorder means for you. The condition still remains a mystery, although an estimated 3 to 6% of Americans, predominantly women, have fibromyalgia syndrome. Even diagnosing the condition can be complex: according to the National Fibromyalgia Association, it can take a patient up to 4 years to be accurately diagnosed.
If you or your loved ones have been diagnosed with fibromyalgia, you may be wondering what the disorder means for you. The condition still remains a mystery, although an estimated 3 to 6% of Americans, predominantly women, have fibromyalgia syndrome. Even diagnosing the condition can be complex: according to the National Fibromyalgia Association, it can take a patient up to 4 years to be accurately diagnosed.
Fibromyalgia is typically diagnosed in patients with:
- Widespread pain in all 4 quadrants of the body for a minimum of 3 months; and
- Tenderness or pain in at least 11 tender points when pressure is applied. These tender points cluster around the neck, shoulder, chest, hip, knee, and elbow regions.
Some fibromyalgia experts say, however, that many people may still have fibromyalgia with fewer than 11 tender points if they have widespread pain and several other common symptoms, including:
- Fatigue
- Sleep disorders
- Chronic headaches
- Dizziness or lightheadedness
- Cognitive or memory impairment
- Malaise and muscle pain after exertion
- Jaw pain
- Morning stiffness
- Menstrual cramping
- Irritable bowels
- Numbness and tingling sensations
- Skin and chemical sensitivities
Correct Diagnosis Is Key
Correct diagnosis of fibromyalgia is very elusive, so if you are diagnosed with the disorder—or suspect that you have it—seek the opinion of more than 1 health care provider. Other conditions may create fibromyalgia- like pain, fatigue, and other symptoms. Ruling other conditions out first is very important. In addition to clinical evaluation that will assess possible causes of your pain, your doctor may need to order blood work to determine if you have:
- Anemia
- Hypothyroidism
- Lyme disease
- Other rheumatic diseases
- Hormonal imbalances
- Allergies and nutritional deficiencies
- Disorders that cause pain, fatigue, and other fibromyalgia-like symptoms.
If the tests show that you have 1 of these conditions, treatment will focus on addressing that problem first. If your pain is caused by a muscle or joint condition, chiropractic care may help relieve it more effectively than other therapies.
Treatment Alternatives
If no underlying cause for your symptoms can be identified, you may have classic fibromyalgia. The traditional allopathic approach includes a prescription of prednisone, anti-inflammatory agents, antidepressants, sleep medications, and muscle relaxants. These temporarily relieve the symptoms, but they do produce side effects. If you prefer a natural approach, the following suggestions may be helpful:
- Studies have shown that a combination of 300 to 600 mg of magnesium per day, along with malic acid, may significantly reduce may significantly reduce the number of tender points and the pain felt at those that remain. B vitamins may also be helpful.
- Eating more omega-3 fatty acids and fewer saturated fats has shown promise in fibromyalgia patients. Limit red meat and saturated fats and increase the amounts of omega-3 fatty acids by including fish, flax, and walnut oils in your diet. Fatty acid deficiencies can interfere with the nervous system and brain function, resulting in depression and poor memory and concentration.
- Improving the quality of sleep can help reduce fatigue. Watch your caffeine intake, especially before going to bed. Reduce TV and computer time. If you watch TV in the evening, choose relaxing, funny programs instead of programs with violent or disturbing content. Ask your doctor of chiropractic for other natural ways to help you sleep better.
- Stress-managing strategies can also help address anxiety or depression issues. Cognitive therapy has been shown helpful in relieving fibromyalgia patients’ negative emotions and depression by changing their perception of themselves and attitudes toward others.
- A traditional gym-based or aerobic exercise program may exacerbate fibromyalgia symptoms and is not recommended. Instead, yoga, Pilates, or tai chi, which offer mild stretching, relaxation, and breathing techniques, may work better than vigorous exercise.
- Chiropractic care has consistently ranked as one of the therapeutic approaches that offer the most relief for the fibromyalgia patient. Your doctor of chiropractic can also include massage therapy, ultrasound, and electrical stimulation in the treatment program, which may help relieve stress, pain, and other symptoms.
Your doctor of chiropractic has the knowledge, training, and expertise to help you understand your problem and, in many cases, to manage it successfully. Remember, however, that the treatment program can be successful only with your active participation. If your doctor of chiropractic feels that he or she cannot help you, you will be directed to another health care provider.
Fight Fatigue
 Fight Fatigue with Nutrition, Activity
Fight Fatigue with Nutrition, Activity
Napoleon Bonaparte once said that courage is only the second virtue in a soldier; the most important one is endurance of fatigue. Nowadays, fighting fatigue has become equally important for a growing army of people too busy or stressed to get adequate rest. In fact, according to a 2007 survey by the National Sleep Foundation (NSF), more than half of American women report getting inadequate sleep. And when too sleepy to function, 66 percent choose to “accept it and keep going.”
Other cultures approach the problem a little differently. Many countries actively practice siesta—a 15- to 30- minute afternoon nap. Several recent studies support the beneficial effect of 10- to 30-minute naps on alertness, performance and learning ability.
Caffeine Quick Fix
In the United States, however, it is caffeine—not naps—that helps 78 percent of people cope with their responsibilities. The benefits of caffeine are real: It improves mood and cognitive performance, and coffee consumption can potentially decrease insulin secretion10 and liver cancer risk. On the negative side, regularly consumed caffeine can increase anxiety, risk of headaches and the inflammation process. Cola beverages, but not coffee, also have been associated with an increased risk of hypertension. Caffeine is considered toxic—causing arrhythmia, tachycardia, vomiting, convulsions, coma or even death—only in amounts exceeding 5g. While the risk of toxicity is rare, the pervasiveness of caffeine warrants some caution. Many soft drinks, for example, contain only between 20 mg and 40 mg of caffeine per an 8-oz can; however, today’s specialty coffees can be very potent—ranging from 58 mg to 259 mg, and even up to 564 mg, per dose.
Food for Energy
Instead of using caffeine to push ourselves to perform despite fatigue, preventing energy drops is a wiser approach, health experts advise. Aside from sleep, our performance—and even our mood—depends on balanced blood sugar levels.
While cautioning against seeking quick blood-sugar boosts, experts recommend juices, such as pomegranate, instead of caffeine or sugar, for those in urgent need of re-energizing.
The key to properly preventing blood-glucose slumps— which can lead to fatigue, headaches, craving sweets, depression, irritability and a host of other symptoms—is the old-fashioned basics of proper nutrition. In one study, a breakfast rich in fiber and carbohydrates caused higher alertness, while high-fat meals led to lower alertness and higher caloric intake throughout the day. Another study showed that protein-rich or balanced meals, which cause less variation in blood glucose levels, improved cognitive performance.
Inadequate glucose is not the only thing contributing to fatigue. It can result from anemia—iron, B12, B6, or folic acid deficiency as well. Omega-3 fatty acids, leafy green vegetables, and vitamins C, E and B12 have been shown to improve memory and cognitive functioning.
Moving the Body
Even with adequate sleep and nutrition, our lack of motion can regularly put us to sleep. To prevent mental fatigue, try starting the day with exercise, taking frequent 5- to 15-second microbreaks (shoulder rolls or stretching) throughout the day, getting up and walking every two hours, and, of course, taking advantage of the lunch break to “do the opposite” of what your job entails. For people with mentally challenging occupations, experts suggest a walk or other physical exercise; for those doing physically taxing work, some brain-stimulating activities, like puzzles.
Imbalanced body postures, such as slouching, also require the body to consume more energy. In addition to adopting an “energy-efficient” standing position, with feet shoulder-width apart, and sitting straight, which helps improve circulation, take frequent 60-second “Stand up, Perk up” breaks that combine relaxation, breathing and stretching.
To those in urgent need of quick re-energizing, consider aerobic exercise instead of coffee. It’s quick and easy—and it stimulates brain chemicals that give us a lift.
Whether re-energizing through sleep, nutrition, exercise or—better yet—a combination of all three, it’s clear that fatigue should not be taken lightly. It’s connected with depression, and antidepressants are now the fastest-growing prescribed class of medications. Instead of taking stimulants, opt for proper exercise, adequate sleep and a balanced diet.
Headaches
If you have a headache, you’re not alone. Nine out of ten Americans suffer from headaches. Some are occasional, some frequent, some are dull and throbbing, and some cause debilitating pain and nausea.
What do you do when you suffer from a pounding headache? Do you grit your teeth and carry on? Lie down? Pop a pill and hope the pain goes away? There is a better alternative.
New research shows that spinal manipulation – the primary form of care provided by doctors of chiropractic – may be an effective treatment option for tension headaches and headaches that originate in the neck.
A report released in 2001 by researchers at the Duke University Evidence-Based Practice Center in Durham, NC, found that spinal manipulation resulted in almost immediate improvement for those headaches that originate in the neck, and had significantly fewer side effects and longer-lasting relief of tension-type headache than a commonly prescribed medication.
Also, a 1995 study in the Journal of Manipulative and Physiological Therapeutics found that spinal manipulative therapy is an effective treatment for tension headaches and that those who ceased chiropractic treatment after four weeks experienced a sustained therapeutic benefit in contrast with those patients who received a commonly prescribed medication.
Headache Triggers
Headaches have many causes, or “triggers.” These may include foods, environmental stimuli (noises, lights, stress, etc.) and/or behaviors (insomnia, excessive exercise, blood sugar changes, etc.). About 5 percent of all headaches are warning signals caused by physical problems.
Ninety-five percent of headaches are primary headaches, such as tension, migraine, or cluster headaches. These types of headaches are not caused by disease. The headache itself is the primary concern.
“The greatest majority of primary headaches are associated with muscle tension in the neck,” says Dr. George B. McClelland, a doctor of chiropractic from Christiansburg, VA. “Today, Americans engage in more sedentary activities than they used to, and more hours are spent in one fixed position or posture. This can increase joint irritation and muscle tension in the neck, upper back and scalp, causing your head to ache.”
What Can You Do?
The ACA suggests the following:
- If you spend a large amount of time in one fixed position, such as in front of a computer, on a sewing machine, typing or reading, take a break and stretch every 30 minutes to one hour. The stretches should take your head and neck through a comfortable range of motion.
- Low-impact exercise may help relieve the pain associated with primary headaches. However, if you are prone to dull, throbbing headaches, avoid heavy exercise. Engage in such activities as walking and low-impact aerobics.
- Avoid teeth clenching. The upper teeth should never touch the lowers, except when swallowing. This results in stress at the temporomandibular joints (TMJ) – the two joints that connect your jaw to your skull – leading to TMJ irritation and a form of tension headaches.
- Drink at least eight 8-ounce glasses of water a day to help avoid dehydration, which can lead to headaches.
What Can a Doctor of Chiropractic Do?
Dr. McClelland says your doctor of chiropractic may do one or more of the following if you suffer from a primary headache:
- Perform spinal manipulation or chiropractic adjustments to improve spinal function and alleviate the stress on your system.
- Provide nutritional advice, recommending a change in diet and perhaps the addition of B complex vitamins.
- Offer advice on posture, ergonomics (work postures), exercises and relaxation techniques. This advice should help to relieve the recurring joint irritation and tension in the muscles of the neck and upper back.
“Doctors of chiropractic undergo extensive training to help their patients in many ways – not just back pain,” says Dr. McClelland. “They know how tension in the spine relates to problems in other parts of the body, and they can take steps to relieve those problems.”
Chiropractic Care Can Help
Talk to your doctor of chiropractic about other ways to improve your lifestyle. Doctors of chiropractic are trained and licensed to examine and treat the entire body with specific emphasis on the nervous and musculoskeletal systems. They can also help people lead healthier lives by focusing on wellness and prevention.
Insomnia
 An old Chinese proverb states, “Only when one cannot sleep does one know how long the night is.” Almost everyone can relate to those words at some point in life. In younger people, stress and worry commonly cause insomnia. Older people suffer from a natural decrease in melatonin—a sleep inducing hormone. Pressures from job and family, illness, side effects of some medications, and aches and pains caused by uncomfortable beds or pillows can also rob us of sleep.
An old Chinese proverb states, “Only when one cannot sleep does one know how long the night is.” Almost everyone can relate to those words at some point in life. In younger people, stress and worry commonly cause insomnia. Older people suffer from a natural decrease in melatonin—a sleep inducing hormone. Pressures from job and family, illness, side effects of some medications, and aches and pains caused by uncomfortable beds or pillows can also rob us of sleep.
Television and computers may also contribute to sleep problems. Computer use, especially in the workplace, has been associated with all types of insomnia in adults—more so than stress, which affects only difficulty falling asleep and early morning arousal. Studies have found that unlimited TV, computer, and Internet use cause sleep deprivation in children—they go to bed later, sleep fewer hours, and feel more tired. Extensive television viewing in adolescence may result in adult sleep problems. Playing computer games may affect adults, as well. A Japanese study found that performing exciting tasks on computers with bright monitors at night affects melatonin concentration and the human biological clock, interfering with sleep.
Overall, 40 million Americans suffer from chronic sleep disorders each year, and an additional 20 million have occasional sleeping problems. Deep sleep helps children grow and improves their learning ability. Lack of sleep affects the immune and nervous systems, memory, judgment, attention, patience, and thinking and reading abilities. It can be especially dangerous for those who drive. The National Highway Traffic Safety Administration estimates that sleep deprivation is responsible for 100,000 vehicle accidents a year, resulting in 1,500 deaths and 71,000 injuries.
Sleeping problems are common in people with most mental disorders, Alzheimer’s, stroke, cancer, and head injury. In hospitalized patients, sleep deprivation may be worsened by treatment schedules and routines. Insomnia contributes to the patients’ confusion, frustration, or depression. They become more sensitive to pain and may request increased pain medications.
Recent research shows that the old advice of sleeping in a comfortable bed in a cool bedroom, eating an early dinner, going to bed at the same time each night, and avoiding caffeine and alcohol before sleep may not work for everyone. Sleep medications are not suitable for long-term use. So, what can we do when all the known remedies have been tried, but sleep is nowhere to be found?
Sleep experts recommend the following:
- On weekends, go to bed at the same time as on weekdays.
- If you exercise in the evening, do so at least 3 hours before bedtime. Also, stay away from evening brain-stimulating or stressful activities, such as balancing checkbooks, reading thrillers, and playing computer games.
- Develop a sleep ritual that will help you to relax and unwind, such as a warm bath.
- Try listening to relaxing music before going to sleep. Soothing music may improve sleep quality in children, older adults, and critically ill patients.
- Limit your child’s exposure to TV or video games to less than 1 hour a day. Long hours spent in front of the TV may lead to not only sleep problems, but also headache, back pain, and eye symptoms. Make sure there is no television set in your child’s bedroom.
- Be sure your children go to bed early and get enough sleep. Children between 3 and 6 years of age should get 11-13 hours of sleep at night. Children from 1st to 5th grade should sleep 10-11 hours. Late bedtimes and short sleeping hours have been strongly associated with childhood obesity.
- Older people should take 30-minute afternoon naps to reduce sleepiness and fatigue and improve mood and performance.
- Sleep on a comfortable, supportive mattress and pillow. Talk to your doctor of chiropractic about choosing the bed and pillow that are right for you.
Researchers are looking into several possible alternative sleeping aids. Although they have not been widely researched, sleep experts agree—it can’t hurt to try
them:
- Acupuncture has been proven effective for some sleep disorders and anxiety.
- Therapeutic touch and relaxing back massage are useful for promoting sleep in critically ill patients. Traditional chiropractic care may also help those with spasms, pain, and joint dysfunction of the neck and back.
Muscle Cramps
 A muscle cramp can bring a jogger to his knees or elicit the fear of drowning in a swimmer; however, athletes are not the only individuals to experience a muscle cramp or spasm. According to one estimate, approximately 95 percent of people will at some time in life experience the sudden, sharp pain associated with a muscle cramp.
A muscle cramp can bring a jogger to his knees or elicit the fear of drowning in a swimmer; however, athletes are not the only individuals to experience a muscle cramp or spasm. According to one estimate, approximately 95 percent of people will at some time in life experience the sudden, sharp pain associated with a muscle cramp.
A muscle spasm is an involuntary contraction of a muscle, part of a muscle, or several muscles that usually act together. If the spasm is forceful and sustained, it becomes a cramp. Most people describe a muscle cramp as a feeling of tightness in the muscle; it’s not unusual to feel a lump of hard muscle tissue underneath the skin in the vicinity of the cramp. During a spasm or cramp, it may be painful, or even difficult, to use the affected muscle or muscle group.
Cramps and spasms can affect any muscle, even those affiliated with the body’s various organs; however, they are most common in the calves, hamstrings, and quadriceps. Cramps in the feet, hands, arms, and lower back occur frequently, as well.
Many possible causes
Common as they are and painful as they can be, a shroud of mystery surrounds the cause of muscle spasms and cramps. Some researchers believe that inadequate stretching and muscle fatigue lead to cramps. According to the University of Michigan, other possible factors include a low level of fitness, overexertion (especially in intense heat), stress, and depletion of electrolytes through excess sweating or dehydration. Certain diuretic medications can also cause cramping due to a loss of sodium, potassium, and magnesium.
Treatment of muscle spasms
Typically, muscle cramps require no treatment other than patience and stretching; medicines are not generally needed to treat an ordinary muscle cramp. Gentle and gradual stretching, along with massage, may ease the pain and hasten recovery.
Some researchers believe that inadequate stretching and muscle fatigue leads to cramps. Other possible factors include a low level of fitness, overexertion, stress, and dehydration.
When a muscle spasm or cramp is the result of an injury, applying ice packs for the first two to three days may help alleviate the pain. Spasms that last a long time may be treated with moist heat for 20 minutes several times a day.
If you tend to get muscle cramps during exercise, make sure you drink enough fluids, and, after your workout, consider a warm Epsom salt bath followed by stretching of the affected muscles. Generally speaking, water is sufficient for rehydration; however, some may find a sports drink or juice beneficial as a means to restore their body’s electrolyte balance.
If your muscle cramps are associated with a specific medical condition, keep in mind that you need to address the underlying health problem for the cramps to subside.
Tips for Prevention
As with any health condition, it is always best to prevent muscle cramps or spasms—especially if you tend to develop them. Consider altering your diet and lifestyle by incorporating the following suggestions:
- Take steps to improve your diet. Eliminate sugar and caffeine from the diet, and increase consumption of fiber and protein. In addition, remember to eat plenty of calcium- and magnesium- rich foods, such as green leafy vegetables, yogurt, legumes, whole grains, tofu, and Brazil nuts. High-potassium foods, including bananas, avocados, lima beans, and fish, may also be helpful.
- Before and after you exercise, stretch muscle groups that tend to cramp.
- Incorporate strengthening exercises into your fitness routine.
- Avoid dehydration. To prevent dehydration, consume plenty of fluids and foods high in water such as fruits and vegetables.
- Avoid excess sodium and soda (high in phosphoric acid), as they can leach calcium.
- Avoid chocolate, caffeine, and alcohol, which can interfere with magnesium absorption.
- Improve your posture. For example, you may have mid-back spasms after sitting at a computer desk for too long in an awkward position.
Vitamin E has been said to help minimize cramp occurrence. Although scientific studies documenting this effect are lacking, anecdotal reports are common and fairly enthusiastic. Since vitamin E is thought to have other beneficial health effects and is not toxic in usual doses, taking 400 units of vitamin E daily could be considered.
Discuss with your doctor of chiropractic if your cramps are severe, happen frequently, respond poorly to simple treatments, or are not related to obvious causes like strenuous exercise. These could indicate a possible problem with circulation, nerves, metabolism, hormones, medications, and/or nutrition.
Neck Pain
 Your neck, also called the cervical spine, begins at the base of the skull and contains seven small vertebrae. Incredibly, the cervical spine supports the full weight of your head, which is on average about 12 pounds. While the cervical spine can move your head in nearly every direction, this flexibility makes the neck very susceptible to pain and injury.
Your neck, also called the cervical spine, begins at the base of the skull and contains seven small vertebrae. Incredibly, the cervical spine supports the full weight of your head, which is on average about 12 pounds. While the cervical spine can move your head in nearly every direction, this flexibility makes the neck very susceptible to pain and injury.
The neck’s susceptibility to injury is due in part to biomechanics. Activities and events that affect cervical biomechanics include extended sitting, repetitive movement, accidents, falls and blows to the body or head, normal aging, and everyday wear and tear. Neck pain can be very bothersome, and it can have a variety of causes.
Here are some of the most typical causes of neck pain:
Injury and Accidents:
A sudden forced movement of the head or neck in any direction and the resulting “rebound” in the opposite direction is known as whiplash. The sudden “whipping” motion injures the surrounding and supporting tissues of the neck and head. Muscles react by tightening and contracting, creating muscle fatigue, which can result in pain and stiffness. Severe whiplash can also be associated with injury to the intervertebral joints, discs, ligaments, muscles, and nerve roots. Car accidents are the most common cause of whiplash.
Growing Older:
Degenerative disorders such as osteoarthritis, spinal stenosis, and degenerative disc disease directly affect the spine.
- Osteoarthritis, a common joint disorder, causes progressive deterioration of cartilage. The body reacts by forming bone spurs that affect joint motion.
- Spinal stenosis causes the small nerve passageways in the vertebrae to narrow, compressing and trapping nerve roots. Stenosis may cause neck, shoulder, and arm pain, as well as numbness, when these nerves are unable to function normally.
- Degenerative disc disease can cause reduction in the elasticity and height of intervertebral discs. Over time, a disc may bulge or herniate, causing tingling, numbness, and pain that runs into the arm.
Daily Life:
Poor posture, obesity, and weak abdominal muscles often disrupt spinal balance, causing the neck to bend forward to compensate. Stress and emotional tension can cause muscles to tighten and contract, resulting in pain and stiffness. Postural stress can contribute to chronic neck pain with symptoms extending into the upper back and the arms.
Chiropractic Care of Neck Pain
During your visit, your doctor of chiropractic will perform exams to locate the source of your pain and will ask you questions about your current symptoms and remedies you may have already tried. For example:
- When did the pain start?
- What have you done for your neck pain?
- Does the pain radiate or travel to other parts of your body?
- Does anything reduce the pain or make it worse?
Your doctor of chiropractic will also do physical and neurological exams. In the physical exam, your doctor will observe your posture, range of motion, and physical condition, noting movement that causes pain. Your doctor will feel your spine, note its curvature and alignment, and feel for muscle spasm. A check of your shoulder area is also in order. During the neurological exam, your doctor will test your reflexes, muscle strength, other nerve changes, and pain spread.
In some instances, your chiropractor might order tests to help diagnose your condition. An x-ray can show narrowed disc space, fractures, bone spurs, or arthritis. A computerized axial tomography scan (a CT or CAT scan) or a magnetic resonance imaging test (an MRI) can show bulging discs and herniations. If nerve damage is suspected, your doctor may order a special test called electromyography (an EMG) to measure how quickly your nerves respond.
Chiropractors are conservative care doctors; their scope of practice does not include the use of drugs or surgery. If your chiropractor diagnoses a condition outside of this conservative scope, such as a neck fracture or an indication of an organic disease, he or she will refer you to the appropriate medical physician or specialist. He or she may also ask for permission to inform your family physician of the care you are receiving to
ensure that your chiropractic care and medical care are properly coordinated.
Neck Adjustments
A neck adjustment (also known as a cervical manipulation) is a precise procedure applied to the joints of the neck, usually by hand. A neck adjustment works to improve the mobility of the spine and to restore range of motion; it can also increase movement of the adjoining muscles. Patients typically notice an improved ability to turn and tilt the head, and a reduction of pain, soreness, and stiffness.
Of course, your chiropractor will develop a program of care that may combine more than one type of treatment, depending on your personal needs. In addition to manipulation, the treatment plan may include mobilization, massage or rehabilitative exercises, or something else.
Neuropathy
The Fire Within
Nerve damage in neuropathy progresses sooner than previously thought, lending urgency to earlier detection and treatment.
By David Glenn
William Loughran retired from his job as a bank director in northeast Maryland in 2014, when he was 68. Like many new retirees, he vowed to ramp up his exercise routine.
“I started going to the gym three or four times a week and walking every day,” he says. “I felt better than I had in years.”
But then, after a long day of walking with his son during a visit to California, it began: “I went to bed, and the soles of my feet felt like they were on fire,” Loughran recalls. “It was jabbing pain, pins-and-needles
pain, and it was pretty severe.”
Within weeks, Loughran’s feet had become so painful that driving his car was a struggle. “Just the slight pressure from the pedals was too much to tolerate,” he says. For months, he spent almost all of his time at
home, in bare feet.
Loughran had developed peripheral neuropathy, a condition shared by hundreds of thousands of Americans. Peripheral neuropathy often begins with damage to the unmyelinated small-fiber nerves, resulting in numbness, tingling and lightninglike shooting pains, most commonly in the feet and hands. The best-known causes of peripheral neuropathy are type 2 diabetes and chemotherapy, but there are several other potential culprits. Vitamin B12 deficiency, high cholesterol, smoking and HIV/AIDS have all been implicated. Roughly one-fifth of peripheral neuropathy cases have no clear cause at all.
After several false starts with physical therapists, podiatrists and other specialists, Loughran realized that
he needed to see a neurologist. He searched online and learned that Johns Hopkins has a prominent research program in peripheral neuropathy.
In early 2016, Loughran found himself in the Johns Hopkins office of Mohammad Khoshnoodi, an assistant professor of neurology. Here at last he received a thorough workup. “Dr. Khoshnoodi did much more extensive blood work than anyone else had done,” Loughran says. “He did nerve conduction studies to see if I had damage to the large-fiber nerves, which I didn’t. And he took three skin biopsies from my leg.” The idea of having skin samples extracted sounded odd at first, Loughran says. But if that was what was required, he was game.
The technique of using skin biopsies to assess peripheral neuropathy was pioneered at Johns Hopkins in the early 1990s by Justin McArthur, who now chairs the Department of Neurology, and the late John Griffin, one of the best-known neurologists in Johns Hopkins history. A major advantage of these biopsies is that they permit objective, quantifiable measurement of nerve damage. They can be taken sequentially from the same sites over a period of months or years, allowing researchers to see exactly how a patient’s nerves and their supporting structures change over time, and how that neurological damage is
affected by changes in the patient’s underlying condition (whether that be diabetes, chemotherapy exposure or something else).
Sequential skin biopsies have become an increasingly powerful tool for uncovering the mysteries of neuropathy. Last spring, Khoshnoodi and five Johns Hopkins colleagues published a much-discussed study in JAMA Neurology that offered some provocative findings. The study considered skin biopsies that were taken sequentially from 52 patients with neuropathy at Johns Hopkins between 2002 and 2010, along with biopsies from 10 healthy volunteers for purposes of comparison.
The study’s first striking finding was that patients with impaired glucose regulation—a condition often known as prediabetes—saw their neuropathies progress just as aggressively as patients with full-blown diabetes. The second finding was that nerve damage increased just as fast at sites on the patients’ upper thighs as it did on patients’ toes and feet, where they actually perceived their symptoms.
“This study reinforces the idea that early neuropathy tends to progress,” says Michael Polydefkis ’93, a professor of neurology and the paper’s senior author. “Primary care doctors should always take it seriously, even if the patient is just talking about slight numbness.”
The fact that prediabetes can cause neuropathies just as severe as full-blown diabetes is relatively well-
known among neurologists and endocrinologists, Khoshnoodi says, but it isn’t sufficiently appreciated by generalist primary care doctors. The sequential skin biopsy study should be a wake-up call, he says. “If we wait until these patients have large-fiber neuropathy, we’ve needlessly lost time and nerve function,” he says. “This is one more reason to be aggressive about controlling patients’ glucose levels.”
Left unattended, Polydefkis says, peripheral neuropathy can advance to more severe kinds of neurological dysfunction, including problems with balance, blood pressure regulation and difficulties in walking. In this study, 14 of 52 patients with small-fiber neuropathy progressed to mild large-fiber neuropathy, meaning that their ankle reflexes were reduced and they were less sensitive to the vibrations of a tuning fork. Such problems are often a prelude to more severe deficits in motion and sensation.
Though Loughran arrived at Johns Hopkins too late to take part in that particular sequential skin biopsy study, the three specimens taken from his ankle confirmed that his skin had a significantly reduced density of small-fiber nerves—the classic sign of small-fiber peripheral neuropathy.
Loughran says he was grateful to have a definitive diagnosis after months of confusion and anxiety. While there are currently no treatments that readily reverse neuropathy in Loughran’s situation, peripheral neuropathy pain can be relieved with various combinations of anti-seizure medications, antidepressants and opioid pain relievers.
None of those drugs can cure the condition or even slow its progression. What can slow neuropathy’s progression—at least for many patients—is correction of the underlying cause. If the patient’s neuropathy is caused primarily by diabetes or prediabetes, strict control of blood glucose levels through diet, exercise and medication can do the trick. If the neuropathy is caused by vitamin B12 deficiency, that is usually simple to correct. If chemotherapy is the villain, the patient and his or her oncologist may want to consider a change in treatment.
“Skin biopsies can tell us exactly how much neuropathy you have, but they don’t tell us anything about the cause,” says Ahmet Hoke, a professor of neurology and another of the study’s authors. “The blood work becomes key. The blood work helps us establish the etiology.”
In Loughran’s case, the blood work strongly suggested prediabetes. He is acting accordingly. “I’ve cut out sodas,” he says, “and I’m trying to get back to exercising.”
For many patients, that last step is easier said than done. “We tell them to exercise,” Polydefkis says, “but exercise can be intolerable because of the burning pain and electric shocks in their feet. That’s why it’s so important to find the right combination of medications to get the neuropathy symptoms under control. Those medicines won’t cure the neuropathy, but they’ll allow patients to be more active, which in turn helps with glucose control when diabetes is a factor.” wimming and other nonweight-bearing exercises are often the best options, Polydefkis adds.
Hoke notes that the sequential skin biopsy study also shed light on the still-unsettled question of why exactly diabetes and prediabetes tend to damage the nerves. Some theories have emphasized the fact that the longest sensory neurons, which extend all the way from the spine to the toes, have huge metabolic needs because of their extreme surface-to-volume ratios. The metabolic dysfunctions associated with diabetes, according to this theory, make it difficult for the long neurons to balance their energy requirements, and they eventually stop working properly. Other scientists have emphasized a simpler, more mechanical model. Diabetes, they say, slowly damages the blood vessels that supply nerves with oxygen and nutrients. Diabetic neuropathy, in this view, is mostly a problem of the vasculature.
The Johns Hopkins studies tend to support the metabolic theory, Hoke and Polydefkis say (though both add that vascular problems probably contribute). “What’s so interesting,” Hoke says, “is that we see damage that is just as bad in prediabetes as in diabetes. That suggests that it isn’t the overall amount of glucose that is causing the neuropathy, but instead that it’s rapid fluctuations in glucose levels. There’s something about those fluctuations that the nerve cells can’t tolerate.”
What about patients who have been diagnosed with diabetes or prediabetes but don’t have any symptoms of neuropathy? “If I were in that situation, I would be vigilant,” Polydefkis says. “There’s reason to believe that nerve damage is already occurring in such patients. I would be very careful about trying to keep my glucose levels stable.”
Osteoarthritis
For decades, osteoarthritis has been considered a part of aging. But not anymore. Recent research points out that older people don’t have to suffer from osteoarthritic pain. And, surprisingly, people much younger than 65 can develop osteoarthritis.
What Is Osteoarthritis?
Osteoarthritis (OA), or degenerative joint disease, affects more than 20 million Americans and is more common in women than in men. The disease affects the cartilage—slippery tissue on the ends of bones that meet in a joint. Normally, cartilage helps bones glide over one another. In an OA patient, however, the cartilage is broken down and eventually wears away. As a result, instead of gliding, bones rub against each other, causing pain, swelling, and loss of motion.
Although the majority of patients with OA are 65 and older, recent research shows that osteoarthritis is not a by-product of aging. Family history of OA, being overweight, lack of exercise, and prior joint injuries are suggested as OA risk factors.
How Is Osteoarthritis Diagnosed?
OA is diagnosed through a combination of clinical history, patient examination, and x-rays. Other tests, such as drawing fluid from the joint, are sometimes used.
The signs of OA include:
- Steady or intermittent joint pain
- Joint stiffness after sitting, sleeping, or otherwise not moving for a long time
- Swelling or tenderness in the joints
- A crunching feeling or the sound of bones rubbing against each other.
If you experience any of these signs, consult your health care provider. While the diagnosis is relatively easy to make, it is often harder to establish whether or not OA causes the patient’s symptoms. That’s why the treating doctor needs to not only make the diagnosis, but also rule out other disorders and conditions that can make the symptoms worse.1 Timely diagnosis and treatment can help manage pain, improve function, and slow the degeneration.
Should Osteoarthritis Patients Exercise?
Exercise is one of the best forms of OA treatment— and prevention. It strengthens the muscular support around the joints and improves and maintains joint mobility and function. In addition, exercise helps control weight and improve the patient’s mood and outlook— important factors influencing the severity of the symptoms.
If you suffer from OA, consider the following exercise tips:
- Low-impact or non-weight-bearing activities, such as walking, stationary training, and light weight training work best for OA patients.
- Use strengthening exercises if the key muscle groups that relate to the function of the joints are weakened by the degeneration.
- If you are overweight, start exercising carefully, so as not to put too much stress on the knee and ankle joints.
- Stair climbing, water aerobics, Theraband workouts, and similar exercises will help to keep the joints mobile without straining them.
- Learn to read the body’s signals and know when to stop, slow down, or rest.
How Can Your Chiropractor Help?
Doctors of chiropractic, by the nature of their work, can detect the earliest degenerative changes in the joints. They see the impact of degenerative changes in the spine, as well as in the hips, knees, and other weight-bearing joints. Doctors of chiropractic are also trained to relieve the pain and improve joint function through natural therapies, such as chiropractic manipulation, trigger-point therapy, or some massage techniques.
Doctors of chiropractic can provide exercise counseling, helping you choose exercises that are best for you. If a sore or swollen joint prevents you from exercising, talk to your doctor of chiropractic about other drug-free pain-relief options, such as applying heat or cold to the affected area. In addition, your doctor of chiropractic can help you choose proper supplements that play important roles in OA prevention and treatment.
Osteoporosis
 Not Just an Elderly Disease
Not Just an Elderly Disease
Osteoporosis has become an epidemic in the United States. About 10 million people—80 percent of them women—suffer from the chronic condition that leads to debilitating and life-threatening fractures. What’s worse, the number of people with low bone mass—high risk for osteoporosis development— keeps growing. While 34 million people now have low bone mass, by 2010, the number is expected to climb to 52 million.
The reasons for the increase are not yet clear, but research points to lifestyle and diet. The bony structure is built in childhood—and weight-bearing physical activity and proper nutrition are essential. Today’s children, however, spend most of their time sitting in front of TV sets or computer monitors and drink calciumrobbing sodas, instead of calcium-rich milk. The inactivity and calcium imbalance makes them more likely to develop osteoporosis.
Osteoporosis Screening
One of the most common bone diseases, osteoporosis is also one of the most preventable. Because osteoporosis is painless until a fracture actually occurs, bone density screening should be used to help diagnose the disease early on. The screening should be done every 2 years, especially in people with the following risk factors for osteoporosis development:
- Female
- Menopausal
- Small frame
- Ovary removal or menopause by age 45
- Prolonged hormonal imbalances
- Known calcium and vitamin D deficiencies
- Insufficient physical activity
- White or Asian ancestry
- Smoker
- Excess caffeine intake (more than 3 cups of coffee, tea or soda a day)
- More than 2 alcoholic drinks per day
- Regular use of certain medications (glucocorticoids, thyroid hormone, anticonvulsants, and aluminum-containing antacids)
- History of eating disorders
- Osteoporosis screening and prevention are especially important because bone loss is irreversible and can only be stabilized, not improved, unless one uses a medication.
The American Chiropractic Association recommends the following tips for preventing and managing osteoporosis:
Exercise
Start a regular exercise program. Exercise puts stress on the bone and helps it strengthen and remodel. Exercise for at least 20 minutes 3 times a week. However, if you have had a fracture, fall frequently, or have osteoporosis, consult with your health care provider before starting any exercise program.
Tai Chi and other weight-bearing activities, such as jogging, walking, stair climbing, playing racquet sports, aerobics, and dancing, can be beneficial. These exercises improve flexibility and balance, reducing the risk of falling and fractures.
Resistance exercises that increase muscle mass and strengthen bones, such as weight lifting, are generally recommended.
Spend time outdoors. Exposure to sunlight increases your level of vitamin D—a necessary element for absorption of calcium, which prevents osteoporosis development.
Safety Precautions
Be careful when bending and lifting heavy objects, including children. When lifting, bend from the knees, not the waist, and try to avoid hunching over while sitting or standing.
Remove throw rugs, electrical cords, and other objects you may trip on from the areas where you walk. Falls from a standing position for an osteoporosis patient often mean fractures.
Nutrition and Supplementation
Decrease consumption of foods high in phosphorus, such as soda, potato chips, hot dogs, bacon, beer, biscuits, crackers, white rice, liver, bologna and peanuts.Too much phosphorus decreases absorption of calcium and other minerals and weakens the bone.
Calcium is essential to building and protecting the bones. Good sources of calcium are milk, cheese, yogurt, broccoli, kale, spinach, and rhubarb. A glass of milk and a cup of yogurt add 600 mg of calcium to your daily diet.
If you are looking for a calcium supplement, try one that’s highly absorbable, such as microcrystalline hydroxyapatite concentrate (MCHC), or one of the malates, fumarates, succinates, glutarates, or citrates. But don’t overdo it. Excess calcium may cause kidney stones, so ask your health care provider about your individual supplement amount.
Check with your health care provider if you are getting enough vitamin D. Without vitamin D, the body won’t absorb calcium.
Pregnancy
Advice for Moms-to-Be
As many new mothers can attest, the muscle strains of pregnancy are very real and can be more than just a nuisance. The average weight gain of 25 to 35 pounds, combined with the increased stress placed on the body by the baby, may result in severe discomfort. Studies have found that about half of all expectant mothers will
develop low-back pain at some point during their pregnancies. This is especially true during late pregnancy, when the baby’s head presses down on a woman’s back, legs and buttocks, irritating her sciatic nerve. And for those who already suffer from low-back pain, the problem can become even worse.
During pregnancy, a woman’s center of gravity almost immediately begins to shift forward to the front of her pelvis. Although a woman’s sacrum—or posterior section of the pelvis—has enough depth to enable her to carry a baby, the displaced weight still increases the stress on her joints. As the baby grows in size, the woman’s weight is projected even farther forward, and the curvature of her lower back is increased, placing extra stress on the spinal disks.
While these changes sound dramatic, pregnancy hormones help loosen the ligaments attached to the pelvic bones. But even these natural changes designed to accommodate the growing baby can result in postural
imbalances.
The American Chiropractic Association recommends the following tips for pregnant women:
- Exercise
Safe exercise during pregnancy can help strengthen your muscles and prevent discomfort. Try exercising at least three times a week, gently stretching before and after exercise. If you weren’t active before your pregnancy, check with your doctor before starting or continuing any exercise program. - Walking, swimming, and stationary cycling are relatively safe cardiovascular exercises for pregnant women because they do not require jerking or bouncing movements. Jogging can be safe for women who were avid runners before becoming pregnant—if done carefully and under a doctor’s supervision.
- Be sure to exercise in an area with secure footing to minimize the likelihood of falls. Your heart rate should not exceed 140 beats per minute during exercise. Strenuous activity should last no more than 15 minutes at a time.
- Stop your exercise immediately if you notice any unusual symptoms, such as vaginal bleeding, dizziness, nausea, weakness, blurred vision, increased swelling, or heart palpitations.
- Health and Safety
Wear flat, sensible shoes. High or chunky heels can exacerbate postural imbalances and make you less steady on your feet, especially as your pregnancy progresses. - When picking up children, bend from the knees, not the waist. And never turn your head when you lift. Avoid picking up heavy objects, if possible.
- Get plenty of rest. Pamper yourself and ask for help if you need it. Take a nap if you’re tired, or lie down and elevate your feet for a few moments when you need a break.
Pregnancy Ergonomics
- Sleep on your side with a pillow between your knees to take pressure off your lower back. Full-length “body pillows” or “pregnancy wedges” may be helpful. Lying on your left side allows unobstructed blood flow and helps your kidneys flush waste from your body.
- If you have to sit at a computer for long hours, make your workstation ergonomically correct. Position the computer monitor so the top of the screen is at or below your eye level, and place your feet on a small footrest to take pressure off your legs and feet. Take periodic breaks every 30 minutes with a quick walk around the office.
Nutrition
Eat small meals or snacks every four to five hours— rather than the usual three large meals—to help keep nausea or extreme hunger at bay. Snack on crackers or yogurt—bland foods high in carbohydrates and protein. Keep saltines in your desk drawer or purse to help stave off waves of “morning sickness.” Supplementing with at least 400 micrograms of folic acid a day before and during pregnancy has been shown to decrease the risk of neural tube birth defects, such as spina bifida. Check with your doctor before taking any vitamin or herbal supplement to make sure it’s safe for you and the baby.
Sacroiliac Joint Dysfunction
 Pain in and around the sacroiliac joint is one of the most common causes of low-back pain. With approximately 80% of the population suffering from low-back pain at some point in their lives, the sacroiliac joint dysfunction (SJD) most likely represents about 15-25% of those cases. SJD is a broad term often applied to the pain in the sacroiliac joint region. While SJD can be painful and debilitating, it is rarely life-threatening, nor does it typically require invasive types of treatment such as surgery.
Pain in and around the sacroiliac joint is one of the most common causes of low-back pain. With approximately 80% of the population suffering from low-back pain at some point in their lives, the sacroiliac joint dysfunction (SJD) most likely represents about 15-25% of those cases. SJD is a broad term often applied to the pain in the sacroiliac joint region. While SJD can be painful and debilitating, it is rarely life-threatening, nor does it typically require invasive types of treatment such as surgery.
What are the sacroiliac joints?
The sacroiliac joints are the largest joints in the spine. If you look at your lower back in a mirror, you will identify these joints as two small dimples on each side of your lower back at the belt line. The joints are found at the base of the spine, between the ilium (the large, flat pelvic bone) and the sacrum (the upside-down triangular bone at the base of the spine). Interestingly, during pregnancy, these ligaments relax to allow the passage of the baby through the birth canal.
Rich with nerves and supported by large, broad ligaments, the long, thin, oblique sacroiliac joints provide stability of the pelvis, absorb shock, and allow just enough motion—a combination of gliding, rotation, and tilting to only a few degrees—to help relieve stress on the spine and hips.
What are the symptoms and causes of sacroiliac joint dysfunction (SJD)?
Symptoms of SJD include low-back pain, typically at the belt line, and pain radiating into the buttock or thigh. These symptoms can often mimic those from other causes of low-back pain, such as disc herniations and disease of the facet joints.
SJD is most common in adults. Most often, SJD is caused by trauma, especially rotation of the joint while the lower back is loaded, as might happen when lifting or participating in some vigorous activity. It is thought that such trauma causes tears, most often small ones, in the ligaments surrounding the joint, resulting in pain and dysfunction. The risk of SJD dysfunction is also thought to increase with true and apparent leg-length inequality, abnormalities in gait, and prolonged exercise. While more serious conditions such as fracture or dislocation, infection, and inflammatory arthritis can cause pain in the sacroiliac joint, minor trauma is a much more common cause.
In pregnant women, SJD is likely secondary to the hormone-induced relaxation of the pelvic ligaments during the third trimester. Weight gain and increased curvature of the lumbar spine are also likely to contribute to the pain in these women.
How is SJD evaluated?
Because SJD pain resembles other types of low-back pain, it is often difficult to isolate it as the actual cause of pain and disability. While no one test is sufficient to diagnose SJD dysfunction, the most commonly used diagnostic procedures are physical examination and anesthetic blocks of the sacroiliac joint. Physical examination procedures, such as orthopedic tests or chiropractic static and motion palpation, involve stressing the joint in various body positions and movements. During anesthetic blocks, a procedure whose validity for SJD diagnosis requires further research, the anesthetic solution often creeps outside the sacroiliac joint and may relieve pain from other structures, making correct diagnosis challenging. Diagnostic imaging procedures, such as x-ray or MRI, aren’t very helpful in evaluating SJD.
How is SJD treated?
Because it is often difficult to isolate the SJD as the source of pain, an appropriate management strategy is hard to implement. It is important for you to choose a doctor who is well-versed in the biomechanics and functions of the sacroiliac joint.
Once the doctor has determined that SJD is the problem, there are myriad therapies available for treatment. Chiropractic manipulation and mobilization of the sacroiliac joint have been demonstrated to be beneficial. In addition, therapeutic exercise can be helpful. These exercise programs should focus on strengthening the core stabilizer muscles of the spine and trunk and also on maintaining the mobility of the sacroiliac joints.
For patients with a leg-length inequality, some type of shoe insert may help manage the problem. These insets can help properly distribute the weight borne by your lower back and sacroiliac joints. If the biomechanics of your gait are abnormal, your doctor may prescribe “gait training.” The doctor will watch you walk and re-train you in proper gait mechanics.
Your doctor may also prescribe a pelvic belt to help stabilize the joints as you perform your daily activities. These belts are thought to reduce the excess rotation that sometimes occurs with SJD.
In some rare cases, more invasive forms of therapy are necessary. These include anesthetic/corticosteroid injections into the sacroiliac joints and/or radiofrequency denervation—a technique in which high-frequency radio waves are used to destroy the nerves in the area of the sacroiliac joints, thereby preventing pain. In severe sacroiliac joint injuries, such as fractures and dislocations, surgery is necessary.
Sciatica
 Sciatica describes persistent pain felt along the sciatic nerve, which runs from the lower back, down through the buttock, and into the lower leg. The sciatic nerve is the longest and widest nerve in the body, running from the lower back through the buttocks and down the back of each leg. It controls the muscles of the lower leg and provides sensation to the thighs, legs, and the soles of the feet.
Sciatica describes persistent pain felt along the sciatic nerve, which runs from the lower back, down through the buttock, and into the lower leg. The sciatic nerve is the longest and widest nerve in the body, running from the lower back through the buttocks and down the back of each leg. It controls the muscles of the lower leg and provides sensation to the thighs, legs, and the soles of the feet.
Although sciatica is a relatively common form of lowback and leg pain, the true meaning of the term is often misunderstood. Sciatica is actually a set of symptoms— not a diagnosis for what is irritating the nerve root and causing the pain.
Sciatica occurs most frequently in people between the ages of 30 and 50 years old. Most often, it tends to mdevelop as a result of general wear and tear on the structures of the lower spine, not as a result of injury.
What are the symptoms of sciatica?
The most common symptom associated with sciatica is pain that radiates along the path of the sciatic nerve, from the lower back and down one leg; however, symptoms can vary widely depending on where the sciatic nerve is affected. Some may experience a mild tingling, a dull ache, or even a burning sensation, typically on one side of the body.
Some patients also report:
- A pins-and-needles sensation, most often in the toes or foot
- Numbness or muscle weakness in the affected leg or foot
Pain from sciatica often begins slowly, gradually intensifying over time. In addition, the pain can worsen after prolonged sitting, sneezing, coughing, bending, or other sudden movements.
What causes sciatica?
The most common cause of sciatica is irritation of the sciatic nerve in the lower back (lumbar region) due to a herniated or ruptured disc. Spinal discs are shock absorbing cushions between each vertebra that keep your spine flexible. Discs have a stronger outer ring and a soft jelly-like center, but as we age, spinal discs can deteriorate, becoming drier, flatter, and more brittle. Frequently, the tough outer covering may develop tiny tears, which allow the jelly-like substance to seep out (rupture or herniation). The herniated disc may then press on the nerve root, causing sciatic symptoms such as pain, tingling, and weakness in the legs and feet. Nerve roots may also be irritated by the chemicals found in the discs’ nucleus.
Other conditions can also put pressure on the nerve, including:
- Spinal stenosis – narrowing of the spinal canal, which places pressure on the spinal cord or the nerve roots
• Degenerative disc disease – a common part of the aging process, leading to a change in the disc shape and function, which can result in disc herniation or pain - Pregnancy – extra weight and pressure on the spine can compress the sciatic nerve
- Trauma – a fall, car accident, or other trauma can injure the nerve roots
- Piriformis syndrome – spasm of the piriformis muscle can compress the sciatic nerve
- Spondylolisthesis – when a vertebra slips forward over another vertebra, the slip can pinch the nerve root
- Spinal tumors or infections – very rare; both can compress the sciatic nerve
In rare cases, a herniated disc may press on nerves that cause you to lose control of bladder or bowel functions. This is an emergency situation and requires an immediate call to your doctor.
How is sciatica diagnosed?
Your doctor of chiropractic will begin by taking a complete patient history. You’ll be asked to describe your pain and to explain when the pain began, and what activities lessen or intensify the pain. Forming a diagnosis will also require a physical and neurological exam, in which the doctor will pay special attention to your spine and legs. You may be asked to perform some basic activities that will test your sensory and muscle strength, as well as your reflexes. For example, you may be asked to lie on an examination table and lift your legs straight in the air, one at a time.
In some cases, your doctor of chiropractic may recommend diagnostic imaging, such as x-ray, MRI, or CT scan. Diagnostic imaging may be used to rule out a more serious condition, such as a tumor or infection, and can be used when patients with severe symptoms fail to respond to six to eight weeks of conservative treatment.
What are my treatment options?
For most people, sciatica responds very well to conservative care, including chiropractic. Keeping in mind that sciatica is a symptom and not a stand-alone medical condition, treatment plans will often vary depending on the underlying cause of the problem.
Chiropractic offers a non-invasive (non-surgical), drug free treatment option. The goal of chiropractic care is to restore spinal movement, thereby improving function while decreasing pain and inflammation. Depending on the cause of the sciatica, a chiropractic treatment plan may cover several different treatment methods, including but not limited to spinal adjustments, ice/heat therapy, ultrasound, TENS, and rehabilitative exercises.
Chiropractic spinal manipulation is proven to be effectiveand has minimal side effects. Recently released practice guidelines published in the Annals of Internal Medicine (2007) stress a conservative approach to treating low-back pain and recommended spinal manipulation as one treatment with proven benefits.
Unless advised otherwise by your doctor of chiropractic, remain active and avoid prolonged bed rest. In the long run, inactivity can make your symptoms worse, whereas regular exercise has been shown to reduce the intensity of pain associated with sciatica.
Fortunately, 80 to 90 percent of patients with sciatica will recover without surgery. If surgery is warranted or your doctor of chiropractic feels it would be best to co-manage your condition with another provider, however, he or she will refer you to a local specialist.
Scoliosis
 Scoliosis affects 5 to 7 million people in the United States. More than a half million visits are made to doctors’ offices each year for evaluation and treatment of scoliosis. Although scoliosis can begin at any age, it most often develops in adolescents between the ages of 10 and 15. Girls are more commonly affected than boys. Because scoliosis can be inherited, children whose parents or siblings are affected by it should definitely be evaluated by a trained professional.
Scoliosis affects 5 to 7 million people in the United States. More than a half million visits are made to doctors’ offices each year for evaluation and treatment of scoliosis. Although scoliosis can begin at any age, it most often develops in adolescents between the ages of 10 and 15. Girls are more commonly affected than boys. Because scoliosis can be inherited, children whose parents or siblings are affected by it should definitely be evaluated by a trained professional.
What is scoliosis?
Because we walk on 2 feet, the human nervous system constantly works through reflexes and postural control to keep our spine in a straight line from side to side. Occasionally, a lateral (sideways) curvature develops. If the curvature is larger than 10 degrees, it is called scoliosis. Curves less than 10 degrees are often just postural changes. Scoliosis can also be accompanied by lordosis (abnormal curvature toward the front) or kyphosis (abnormal curvature toward the back). In most cases, the vertebrae are also rotated.
In more than 80% of cases, the cause of scoliotic curvatures is unknown; we call this condition idiopathic scoliosis. In other cases, trauma, neurological disease, tumors, and the like are responsible. Functional scoliosis is often caused by some postural problem, muscle spasm, or leg-length inequality, which can often be addressed. Structural scoliosis does not reduce with postural maneuvers. Either type can be idiopathic or have an underlying cause.
What are the symptoms of scoliosis?
Scoliosis can significantly affect the quality of life by limiting activity, causing pain, reducing lung function, or affecting heart function. Diminished self-esteem and other psychological problems are also seen. Because scoliosis occurs most commonly during adolescence, teens with extreme spinal deviations from the norm are often teased by their peers. Fortunately, 4 out of 5 people with scoliosis have curves of less than 20 degrees, which are usually not detectable to the untrained eye. These small curves are typically no cause for great concern, provided there are no signs of further progression. In growing children and adolescents, however, mild curvatures can worsen quite rapidly—by 10 degrees or more—in a few months. Therefore, frequent checkups are often necessary for this age group.
How is scoliosis evaluated?
Evaluation begins with a thorough history and physical examination, including postural analysis. If a scoliotic curvature is discovered, a more in-depth evaluation is needed. This might include a search for birth defects, trauma, and other factors that can cause structural curves.
Patients with substantial spinal curvatures very often require an x-ray evaluation of the spine. The procedure helps determine the location and magnitude of the scoliosis, along with an underlying cause not evident on physical examination, other associated curvatures, and the health of other organ systems that might be affected by the scoliosis. In addition, x-rays of the wrist are often performed. These films help determine the skeletal age of the person, to see if it matches an accepted standard, which helps the doctor determine the likelihood of progression. Depending on the scoliosis severity, x-rays may need to be repeated as often as every 3 to 4 months to as little as once every few years.
Other tests, including evaluation by a Scoliometer™, might also be ordered by the doctor. This device measures the size, by angle, of the rib hump associated with the scoliosis. It is non-invasive, painless, and requires no special procedures. A Scoliometer™ is best used as a guide concerning progression in a person with a known scoliosis—not as a screening device.
Is scoliosis always progressive?
Generally, it is not. In fact, the vast majority of scolioses remains mild, is not progressive, and requires little treatment, if any.
In one group of patients, however, scoliosis is often more progressive. This group is made up of young girls who have scolioses of 25 degrees or larger, but who have not yet had their first menstrual period. Girls generally grow quite quickly during the 12 months before their first period and if they have scolioses, the curvatures tend to progress rapidly. In girls who have already had their first periods, the rate of growth is slower, so their curves tend to progress more slowly.
What is the treatment for scoliosis?
There are generally 3 treatment options for scoliosis— careful observation, bracing, and surgery. Careful observation is the most common “treatment,” as most mild scolioses do not progress and cause few, if any, physical problems. Bracing is generally reserved for children who have not reached skeletal maturity (the time when the skeleton stops growing), and who have curves between 25 and 45 degrees. Surgery is generally used in the few cases where the curves are greater than 45 degrees and progressive, and/or when the scoliosis may affect the function of the heart, lungs, or other vital organs.
Spinal manipulation, therapeutic exercise, and electrical muscle stimulation have also been advocated in the treatment of scoliosis. None of these therapies alone has been shown to consistently reduce scoliosis or to make the curvatures worse. For patients with back pain along with the scoliosis, manipulation and exercise may be of help.
Most people with scoliosis lead normal, happy, and productive lives. Physical activity including exercise is generally well-tolerated and should be encouraged in most cases.
Spinal Disc Problems
Eighty percent of people experience back pain, and at any one point in time, approximately 20% of the population has back pain. For many decades, doctors and scientists believed that most back pain was caused by “slipped” or “torn” discs. We now know this not to be true. Disc problems constitute only a small portion of the causes of back pain and rarely require surgery for pain relief.
What are spinal discs?
Spinal discs are a critically important part of your spinal column. Along with the vertebrae, also called the spinal bones, they perform many functions. The discs provide shock absorption, protecting the spinal cord and ensuring flexibility of the spine. They also perform other functions.
The spinal discs are essentially ligaments (structures connecting bones) that attach to the top and bottom of each vertebra. They are thick, ligament-like outer rings, also known as annuli fibrosis. Because they are arranged in an alternating pattern with the vertebrae, annuli fibrosis allow flexibility while preventing the vertebrae from moving too much and causing injury. Inside a single annulus fibrosis is a jelly-like substance called the nucleus pulposis. It contains some proteins, but is primarily made up of water. The nucleus provides more shock absorption than does the annulus, and it also acts as a fulcrum to direct the type of movement through which each vertebra travels.
What are the most common disc problems?
- A disc “bulge” results from slight tears in the outermost fibers of an annulus fibrosis. These small tears can be painful for a short time.
- A disc protrusion/extrusion, also called “herniation,” is a more significant injury. It results from a complete or significant tear of the fibers of an annulus-when some of the nucleus leaks through. A herniation can also be painful and may even cause nerve compression. In the most severe cases, the spinal cord can become compressed.
- The most common disc problem suffered by adults is degenerative disc disease. This occurs when the nucleus loses water and small tears develop in it. The body then forms osteophytes (bone spurs), along the edges of the vertebra and the disc space narrows. We used to believe that this was a function of “wear and tear” as we aged. The most recent evidence shows that, most often, there is a hereditary link to the development of degenerative disc disease. Degenerative disc disease can also be caused by trauma/injury.
What are the common signs and symptoms of disc problems?
Common signs of disc problems include, but are not limited to:
- Back or neck pain
- Leg or arm pain
- Stiffness
- Tenderness of the spine and spinal muscles
How are disc problems diagnosed?
Disc problems are most often diagnosed with the use of a thorough history and physical examination, including examination of your nervous and musculoskeletal systems. Your doctor will most likely move your back and arms and legs into various positions while applying pressure to your joints.
Plain film x-rays are helpful in only some forms of disc problems. Magnetic resonance imaging (MRI) hasbecome the mainstay for the diagnosis of disc problems, as it images the discs quite nicely. Your doctor may order an MRI if he or she feels it would be helpful in diagnosing a disc problem and determining the proper course of care for you. Most often, however, this is not necessary.
How are disc problems treated?
Luckily, in most circumstances, disc problems are easily treated with conservative interventions. Early in the course of an acute injury, your doctor of chiropractic will very likely set a goal of pain control, using several different physical modalities to reach it. Both ice and heat have shown effectiveness in managing the pain of acute low-back injury. Your doctor of chiropractic will help you determine which is most effective for you.
In addition, getting you back on your feet and moving as quickly as is safely possible is critical. Typically, the less time you spend in bed, the better off you are in terms of long-term results. You’ll also need to learn not to be afraid to move. If you “baby” your back, in most cases, the long-term results will be worse.
Chiropractic spinal manipulation has also been demonstrated to be a safe and effective tool in the management of disc problems. Manipulation is especially effective when combined with therapeutic exercise. In most circumstances, spine surgery and injections are not necessary in the management of disc problems-and they often cause more problems than they’re worth. Your doctor of chiropractic will discuss all available treatment options with you and help you decide on the best course of action.
Can disc problems be prevented?
Recent scientific evidence suggests that the best way to prevent back pain, including disc injury-related back pain, is to stay physically active and exercise regularly. This generally means performing general fitness exercises, such as walking, running, and swimming. There is no solid scientific evidence, however, to suggest that any particular exercises designed to strengthen the back are more useful than others. Your doctor of chiropractic can design a specific exercise regimen to fit your needs.
It is also critically important to have “spinal awareness.” Make a conscious effort, for example, to be aware of what posture you are maintaining when you sit, stand, lie down, work, and exercise. Lift objects with proper posture, including bending your knees, keeping the object close to your body, keeping your back straight and lifting with your legs. Never lift an object by bending over and twisting. You’ll only invite a back injury.
Temporomandibular Joint Disorder
Does it hurt when you chew, open wide to yawn or use your jaws? Do you have pain or soreness in front of the ear, in the jaw muscle, cheek, the teeth or the temples? Do you have pain or soreness in your teeth? Do your jaws make noises loud enough to bother you or others? Do you find it difficult to open your mouth
wide? Does your jaw ever get stuck/locked as you open it?
If you answered “yes” to some of these questions, you may have a temporomandibular joint disorder, or TMD.
TMD is a group of conditions, often painful, that affect the jaw joint. Signs may include:
- Radiating pain in the face, neck, or shoulders;
- Limited movement or locking of the jaw;
- Painful clicking or grating when opening or closing the mouth;
- A significant change in the way the upper and lower teeth fit together;
• Headaches, earaches, dizziness, hearing problems and difficulty swallowing. - For most people, pain or discomfort in the jaw muscles or joints is temporary, often occurs in cycles, and resolves once you stop moving the area. Some people with TMD pain, however, can develop chronic symptoms. Your doctor of chiropractic can help you establish whether your pain is due to TMD and can provide conservative treatment if needed.
What Causes TMD?
Researchers agree that TMD falls into three categories:
- Myofascial pain—discomfort or pain in the muscles of the jaw, neck, and shoulders;
- A dislocated jaw or displaced disc;
- Degenerative joint disease—rheumatoid arthritis or osteoarthritis in the jaw joint.
Severe injury to the jaw is a leading cause of TMD. For example, anything from a hit in the jaw during a sporting activity to overuse syndromes, such as chewing gum excessively or chewing on one side of the mouth too frequently, may cause TMD.
Both physical and emotional stress can lead to TMD, as well. The once-common practice of sitting in a dentist’s chair for several hours with the mouth wide open may have contributed to TMD in the past. Now, most dentists are aware that this is harmful to the jaw. In addition to taking breaks while they do dental work, today’s dentists also screen patients for any weaknesses in the jaw structure that would make physical injury likely if they keep their mouths open very long. In that case, they may use medications during the procedure to minimize the injury potential, or they may send the patient to physical therapy immediately after treatment. In less severe cases, they instruct patients in exercises they can do at home to loosen up the joint after the visit.
While emotional stress itself is not usually a cause of TMD, the way stress shows up in the body can be. When people are under psychological stress, they may clench their teeth, which can be a major factor in their TMD.
Some conditions once accepted as causes of TMD have been dismissed—moderate gum chewing, nonpainful jaw clicking, orthodontic treatment (when it does not involve the prolonged opening of the mouth, as mentioned above), and upper and lower jaws that have never fit together well. Popular theory now holds that while these may be triggers, they are not causes.
Women experience TMD four times as often as men. Several factors may contribute to this higher ratio, including sitting too long at the workplace, general posture and higher heels.
TMD Diagnosis and Treatment
To help diagnose or rule out TMD, your doctor of chiropractic (DC) may ask you to put three fingers in your mouth and bite down on them. You may also be asked to open and close your mouth and chew repeatedly while the doctor monitors the dimensions of the jaw joint and the balance of the muscles. If you have no problems while doing these things, then the problem is not likely to be TMD. Your DC can then look for signs of inflammation and abnormalities. Sometimes special imaging, an x-ray or an MRI may be needed to help confirm the diagnosis.
If you have TMD, your doctor may recommend chiropractic manipulation, massage, applying heat/ice and special exercises. In most cases, your doctor’s first goal is to relieve symptoms, particularly pain. If your doctor of chiropractic feels that you need special appliances or splints (with the exception of the “waterpack” and other guards against teeth grinding), he or she will refer you to a dentist or orthodontist for cocomanagement. In addition to treatment, your doctor of chiropractic can teach you how to:
- Apply heat and ice to lessen the pain. Ice is recommended shortly after the injury or after your pain has started. In the later stages of healing, you need to switch to heat, especially if you are still experiencing discomfort.
- Avoid harmful joint movements. For example, chomping into a hard apple is just as bad as crunching into hard candy (some hard candies are even called “jawbreakers”—for good reason). And giant sandwiches can cause the mouth to open too wide and have a destabilizing effect on the jaw.
- Perform TMD-specific exercises. Depending on your condition, your DC may recommend stretching or strengthening exercises. Stretching helps to loosen tight muscles and strengthening helps to tighten muscles that have become loose. Special feedback sensors in the jaw can be retrained, as well, if needed.
Thoracic Outlet Syndrome
The thoracic outlet is a small space between the collarbone (clavicle) and the first rib. Thoracic outlet syndrome (TOS) is a group of disorders that involve compression, injury, or irritation of the nerves, blood vessels, or veins in the thoracic outlet. This can cause pain in the shoulders and neck and numbness in the fingers.
The cause of the compression can vary and may include:
- Anatomical defects: Inherited defects present at birth, including a cervical rib—an extra rib located above the first rib—or an abnormally tight fibrous band connecting the spine to the rib.
- Poor posture: Drooping the shoulders or holding the head in a forward position can cause compression in the thoracic outlet area.
- Trauma: A traumatic event, such as a car accident, can cause internal changes that then compress the nerves in the thoracic outlet.
- Repetitive activity: Doing the same activity over and over can wear on the body’s tissues. You may notice symptoms of thoracic outlet syndrome if your job requires continuous repetition of a movement, such as typing on a computer for extended periods, working on an assembly line, or stocking shelves and repeatedly lifting things above your head.
Another cause is the carrying of heavy shoulder bags or briefcases. In some cases, your health care provider may not be able to determine the exact cause of symptoms.
What Are the Symptoms of TOS?
The symptoms of thoracic outlet syndrome—as well as the intensity of any symptoms—vary between individuals and depend on the location of the compression site. When nerves are compressed, signs and symptoms often include:
- Numbness or tingling in the neck, shoulder, arm, or fingers
- An ache in the arm or hand
- Weakening grip
- Difficulty with fine-motor tasks
Compression of one or more veins and arteries can result in symptoms such as:
- Bluish discoloration of the hand
- Swelling or puffiness in the arm or hand
- Coldness of hands or fingers
- Throbbing lump near the collarbone (clavicle)
- Deep pain in the neck and shoulder region that may increase at night
- Easily fatigued arms and hands
Diagnosis and Treatment of TOS
Because TOS doesn’t have unique symptoms, it can be difficult to diagnose. A detailed health history and thorough physical examination are the most important components in establishing the diagnosis of TOS. Your doctor of chiropractic may also recommend X-rays, MRI (magnetic resonance imaging), laboratory tests, or a nerve conduction velocity test if he or she suspects TOS. It is important for your provider to differentiate TOS from other conditions, such as carpal tunnel syndrome, shoulder tendinitis, and a herniated cervical disc—just to name a few of the many conditions that can cause signs and symptoms.
In the vast majority of neurological TOS cases, a conservative, non-surgical approach to treatment is most effective, especially when the condition is diagnosed early. A chiropractic treatment plan for TOS may include a mix of joint mobilization/manipulation, physical therapy modalities, home stretching exercises, and soft-tissue therapy.
Patients should avoid prolonged positions that cause them to hold their arms out or overhead. For example, avoid sleeping with the arm extended up behind the head. It is also helpful to have rest periods at work to minimize fatigue. Weight reduction can be helpful for obese patients. Patients should avoid sleeping on the stomach with arms above the head. They should also avoid repetitively lifting heavy objects.
Home Exercises
A home exercise program can be a very valuable aspect of any TOS treatment plan. Below are a few stretching exercises. All of these exercises should be performed slowly and carefully. Each position is taken to the point where a stretch, but no pain, is felt. Patients should not bounce to increase the length of their stretches in any of these positions.
Corner Stretch — Stand facing the corner of the room (about one foot from the corner) with your hands at shoulder height, one on each wall. Lean into the corner until you feel a gentle stretch across your chest. Hold for five seconds.
Neck Stretch — Stand tall with your arms at your side. Bend your head to the left and try to touch your left ear to your left shoulder. Do not move your shoulders as you do this. Hold for five seconds. Repeat on the other side.
Shoulder Rolls — Stand tall with your arms relaxed at your sides. Shrug your shoulders forward and up. Relax. Shrug your shoulders backward and up. Relax. Shrug your shoulders straight up. As you get stronger, you can hold 5- to 20-lb. weights in each hand while conducting the shoulder exercises.
Thoracic Extension — Lie face down. Clasp your hands behind your back. Lift your head and chest off the floor as high as you can while squeezing your shoulders blades together and tucking in your chin. Hold this position for a count of three seconds. Exhale as you return to the starting position.
Overhead Raise — Stand tall with your arms straight out from your sides at shoulder level and with a 2-lb. weight in each hand. Raise your arms until they meet over your head. Relax and repeat. Keep your elbows straight and maintain the position of the palms (the backs of the hands should approach one another, not the palms) while you are doing this exercise. Note: As strength improves, the weights should be made heavier, increasing to 5 to 10 lbs.